Knee Surgery & Rehabilitation
Over 120,000 ACL reconstructions are performed in the United States each year. Because many people never seek a physician’s care after they hurt their knee, it is estimated that the number of new ACL reconstructions is at least double that amount. Certainly, ACL ruptures are one of the most common serious knee injuries that occur and the consequences can be devastating to both young and older individuals alike.



Why Choose NKI for your ACL Reconstruction
For certain patients in whom multiple ligaments are ruptured, an allograft (or transplant) may be required. We use only grafts from tissue banks that have undergone FDA inspections and are certified by the American Association of Tissue Banks.
Frequently Asked Questions
ACL Reconstruction What you need to know:
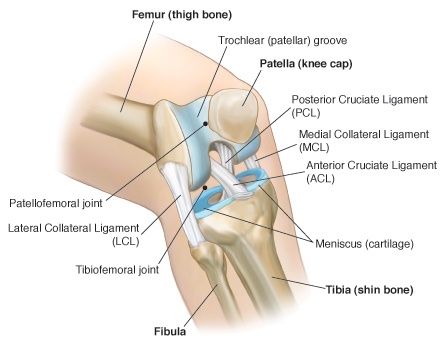
What is the ACL?
The anterior cruciate ligament (ACL) is one of four main ligaments that holds the femur and tibia together. The ACL’s job is to keep the tibia from coming too far forward and/or rotating away from the femur.
The ACL is like a piece of rope. When it is stretched beyond its ability to work, the rope fibers tear or are torn apart. Treatment options are based on whether the ACL is partially torn or completely torn apart.
How do I know if I’ve torn my ACL?
Most people have the following symptoms:
- Distinctive “pop” heard during the injury
- Swelling either right away or within a few hours of the injury
- Loss of ability to extend and flex the knee
- “Giving-way” episodes. Your knee may collapse and you fall to the ground
- Pain
- Some people are able to continue their activity; some people’s knees collapse and they cannot walk normally
You may also experience:
- Knee “catching” or “locking”. If your knee gets stuck in position, you may also have a meniscus tear.
*Swelling and loss of motion are the two biggest clues pointing to a torn ACL
When should I see a physician?
If your symptoms last more than two days, you should seek the proper medical care; a sports medicine trained physician. If your pain and swelling are severe immediately after the injury, seek attention in an emergency room to make sure a fracture has not occurred. Even if you have a partial ACL tear, we recommend that you see a sports medicine physician who will provide a proper diagnosis. Approximately 50-60% of people who have an ACL tear also have a meniscus tear. If you have a meniscus tear, your knee is probably catching or locking, indicating that the meniscus is “flipped up into the joint” preventing knee motion.
Why should I see a sports medicine-trained orthopaedic surgeon?
The training of an orthopaedic surgeon involves many years of undergraduate, medical school, and residency education. The specialization of sports medicine involves additional training, usually at an educational center where a fellowship year is completed. This involves advanced training in arthroscopic surgery, required in the treatment of most knee, shoulder, ankle, elbow and sports medicine-related injuries. The sports medicine-trained surgeon also has knowledge of specific rehabilitation and muscle performance issues to safely regain function and return patients to athletics. A sports medicine center combines the disciplines of physicians, physical therapists, athletic trainers, and more to totally heal all aspects of an injury.
Will I Need Surgery?
There are four factors that determine the answer to that question.
The answer is “no” if:
You have a sedentary lifestyle requiring no particularly strenuous activity; then you may not need surgery. However, that does not mean you should not seek treatment. Conservative treatment does not mean no treatment. You must still be under an orthopaedic surgeon’s care and go through rehabilitation to strengthen your knee. If not, you may have additional “giving-way” episodes which continue to damage the structures in the knee, causing arthritis. Ultimately we want to prevent arthritis.
The answer is an immediate “yes” if:
Your knee is locking or catching, several times daily. As we mentioned above, you may also have a meniscus tear. This is the only time you will require surgery within a few days after your injury. A meniscus tear needs to be repaired immediately if it is causing your knee to catch or lock.
The answer is also “yes” if:
You are an active person or have a physically demanding occupation, we suggest you have your ACL reconstructed. We have a 95% success rate with ACL reconstructions. Advances in surgical techniques and rehabilitation have made the surgery appropriate and successful for all physically active individuals, not just the highly competitive athletes.
Before you can have surgery, several things will need to happen:
-
Knee swelling must be eliminated
-
You must go through 2 to 4 weeks of rehabilitation to regain joint motion and muscle function after the injury. It is easy to lose muscle very quickly. Rehabilitation focuses teaching important exercises to regain muscle strength in addition to mental preparation for the surgery. Though an ACL reconstruction is a relatively common procedure, with more than 50,000 performed each year, it is still major surgery. The stronger your knee and attitude before surgery, the better your surgical outcome will be.
The answer is also “yes” if:
You continue to have “giving-way” episodes. Repeated instances, when your knee gives-way and you fall to the ground, indicate you have a chronic knee problem. Surgical repair of the ACL can prevent future damage to the knee joint and resulting arthritis. It can also improve your quality of life.
What Are My Surgical Options?
At the Noyes Knee Institute, we prefer to use autograft tissue (taken from your own body) for most ACL reconstructions. There are three autograft tissue options that provide strength and viability equal to or greater than the ACL:
-
Patellar Tendon
-
Semitendinosus and Gracilis (hamstring) Tendons
-
Quadriceps Tendon
Our physicians are also well-experienced with the implantation of allograft tissues (taken from a cadaver donor). We only use allograft tissues from tissue banks that are certified by the American Association of Tissue Banks and have passed FDA inspection. The allografts are irradiated to kill bacteria and many viruses. The level of irradiation (2.5 megarads) does not harm the biomechanical properties or healing capabilities of the allograft tissues. We use two types of allografts for ACL reconstruction::
-
Patellar Tendon
-
Achilles Tendon
Most surgeons recommend the procedure they are most comfortable with and have used the most frequently. We are fortunate at Cincinnati Sportsmedicine that we have a wide range of experience with all types of grafts and can recommend the one best suited for each individual patient.
A tremendous amount of research data exists on the outcome of each type of graft used for ACL reconstruction. In our extensive clinical studies, we have found that patellar tendon and hamstring tendon autografts have a higher success rate than allografts and that is why these are our preferred grafts for most patients. The exceptions are patients who have multiple ligaments that are ruptured and in whom autograft tissues are not available or feasible to use. Some patients who have had a prior ACL reconstruction which failed may be considered candidates for allograft reconstruction, especially if other ligaments also require surgical correction at the same time.
What Can I Expect Following My Surgery?
Rehabilitation is an essential element or your recovery. The success of your ACL surgery is not only determined by an expert surgeon, but also by following a rigorous rehabilitation program. YOUR SURGERY MAY FAIL IF YOU DO NOT FOLLOW THE RIGHT REHABILITATION PROGRAM.
There are two rehabilitation protocols we follow.
- Early Return to Strenuous Activities Protocol
This rehabilitation program is designed for patients who have had an ACL reconstruction and have had no other surgical procedures, such as a complex meniscus repair. They do not have knee arthritis or damage to their joint lining. They have a “normal” joint and are highly competitive athletes who want to return to their sport ASAP.
This program involves:
- Immediate motion and exercises following surgery
- Limited use of crutches, for comfort only
- Possible running as early as 12 weeks after surgery*
- Full sports activity resumed as early as 6 months after surgery*
*Only if certain muscle strength, ligament function, neuromuscular, and symptom criteria are met. Patients undergo rigorous testing and training before full sports are allowed.
- Protocol for Revision, Allografts, Complex Knees
This rehabilitation program is for everyone else. If you have had other major operative procedures, in addition to your ACL repair or if arthritis was discovered during the initial diagnostic arthroscopy.
This program involves:
- Immediate motion and exercises following surgery
- Crutches for approximately 5-6 weeks
- Running, if desired, six months after surgery**
- Return to sports activity, if desired, 7-12 months after surgery**
***Only if certain muscle strength, ligament function, neuromuscular, and symptom criteria are met. Patients undergo rigorous testing and training before full sports are allowed. Patients with arthritis are usually advised to return only to light recreational activity to avoid further joint damage.
Click here to see our detailed ACL Recon Delayed rehabilitation protocol.
How do I avoid complications after surgery?
The Noyes Knee Institute ACL Reconstruction Program has one of the lowest complication rates reported to date in the medical literature. Two Noyes Knee Institute studies, some of the medical community’s largest on ACL complications, support our claim that our surgical techniques, followed by our rehabilitation programs are the most successful in the country. Expertise of the surgeon in understanding how to correctly place each graft, combined with the right rehabilitation program is based on a concept developed by Dr. Frank R. Noyes more than 25 years ago. The principles involve immediate knee motion, early functional use of the knee, early intervention with rehabilitation techniques if motion or strength is limited, allowing time for healing, maximizing neuromuscular training, and graduated return to high intensity sports to avoid injury.
What if after my surgery, I’m still having problems with my knee?
If your knee is loose and unstable, you continue to have pain, swelling, and giving-way, and you’ve already had an ACL reconstruction, then your surgery may have failed. An ACL reconstruction fails for many reasons – fortunately, this occurs in only about 5% of patients. You should seek treatment with a center and orthopaedic surgeon highly trained and experienced with ACL revision surgery. We see patients from around the world who have had prior knee surgery and problems have occured. With our extensive experience, we have developed procedures, techniques, and rehablitation programs that are specially designed to help patients still attempt to achieve a good result.