Knee Surgery & Rehabilitation
Although tremendous advances have been achieved in reconstructing the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), and lateral collateral ligament (LCL), these operations may fail to restore normal knee stability for a variety of reasons.
ACL reconstruction is a popular operation which is performed on over 100,000 patients in the United States each year. Although operative techniques, graft substitutes, and rehabilitation programs continue to improve, ACL reconstructions fail because of many reasons. This results in knee pain and instability. Thousands of individuals may require an ACL revision operation each year in the U.S. alone.

Why Choose NKI for your Knee Ligament Revision
Dr. Frank Noyes and researchers at the Noyes Knee Institute have spent over three decades studying the causes of failure of knee ligament reconstructions, and the outcome of revision operations using a variety of graft materials. Few institutions in the country have the experience found at the Noyes Knee Institute in handling this problem. From the diagnosis of the factors that caused the operation to fail, to the advanced surgical options, and finally the comprehensive rehabilitation problem, we offer hope for even the most difficult knee problems.
Frequently Asked Questions
ACL Reconstruction What you need to know:
Why do ACL reconstructions fail?
- Use of a graft that is biomechanically inferior to the native ACL
- Failure of the graft to complete the process of healing (also referred to as ligamentization)
- Improper placement or orientation of the graft tunnels, usually in either a vertical or anterior position, which does not replicate normal ACL anatomy
- Impingement of the graft in the femoral notch due to inadequate notchplasty or graft placement
- Improper tensioning of the graft before fixation
- Inadequate graft fixation because of either the fixation device itself or inadequate bone stock of the host bone (known as osteopenia)
- Failure to correct associated knee ligament ruptures or deficiencies, commonly involving the posterolateral structures
- Failure to correct a bowed leg condition (known as varus osseous lower limb malalignment)
- Traumatic reinjury
- A combination of any of the above factors
Shown below is an x-ray of a patient 1 year after an ACL reconstruction was done with a patellar tendon autograft. The operation failed because the graft tunnels were placed too far anteriorly.

Shown below is an x-ray of the same patient that was taken after an ACL revision reconstruction was performed with a quadriceps tendon autograft. The screw in the femur from the first procedure was placed so deeply and away from the new tunnel that id did not require removal.

Who are candidates for an ACL revision operation?
Patients who are considering revision reconstruction at the NKI must undergo a comprehensive evaluation by the surgeon that includes a meticulous physical examination; observation of gait during walking to identify problems that require correction before surgery; and analysis of x-ray and MRI films to determine the location and size of the prior graft tunnel, joint narrowing (indicating arthritis), and overall lower limb alignment.
- Patients who have sustained complete failure of a prior ACL procedure as determined by a fully positive pivot-shift test and > 6 mm of increased anterior tibial translation on Lachman or instrumented KT-2000 testing
- Patients who have sustained complete failure of a prior ACL procedure and have symptoms or functional limitations with daily or sports activities
Who are NOT candidates for an ACL revision procedure?
- Patients with partial function of a prior ACL reconstruction
- Patients who do not have symptoms (pain, swelling, giving-way) with activities
- Patients who had a prior joint infection
- Patients who are obese (body mass index > 30)
- Patients who have bowed legs that will not undergo a high tibial osteotomy before or with the ACL revision reconstruction
- Patients with severe muscle atrophy
- Patients with poor motivation or unrealistic expectations
- Patients who have knee arthrofibrosis
- Patients who have deficiency of the posterolateral structures and will not undergo an associated posterolateral reconstruction with the ACL revision
What is the preferred graft for ACL revision reconstruction?
Our first graft choice is the patellar tendon autograft. Studies show that this graft appears to have acceptable results in terms of restored knee stability. If the patellar tendon was previously used, then the opposite knee provides an excellent source to obtain the portion of this tendon required for the operation. There does not appear to be a negative effect on patient recovery when the patellar tendon is harvested from the opposite knee.
At the NKI, this graft is harvested with a very small (1 inch) incision, the patellar tendon is carefully sutured back together, and the defect created in the patella is filled in with bone obtained during other portions of the operation. These technical aspects of the operation, along with a carefully designed rehabilitation program, reduce graft site pain and enable patients to kneel after a few months.
In patients who will not consider harvest of the patellar tendon from the opposite knee, the quadriceps tendon is a reasonable graft source according to its size and structural properties. A semitendinosus-gracilis four-strand (hamstring) autograft may be considered if the tibial and femoral tunnels are not enlarged and if there is no loss of bone stock at the prior tibial or femoral graft sites. In our experience, this is a rare graft option for ACL revision, especially in female athletes who usually have weak hamstring muscles and in whom the harvest of this graft would result in a permanent deficit in hamstring strength.
Allografts have been used in revision ACL cases, but because they have a higher failure rate (compared to autografts), they are considered our last graft option.
What is the rehabilitation program after ACL revision reconstruction?
For patients who undergo ACL revision without an associated posterolateral reconstruction or high tibial osteotomy at the NKI, the postoperative rehabilitation protocol may be found by clicking here.
For patients who undergo ACL revision with an associated posterolateral reconstruction at the NKI, the postoperative rehabilitation protocol may be found by clicking here.
For patients who undergo ACL revision with a high tibial osteotomy at the NKI, the postoperative rehabilitation protocol may be found by clicking here.
What are the results of ACL revision reconstruction?
The results of ACL revision are based on other operative procedures that are required and the condition of the menisci and articular cartilage. Because the results of ACL revision are generally reported to be less favorable compared to those of primary (first-time) procedures, the decision to proceed must be carefully discussed by the surgeon and patient.
The outcome of ACL revision reconstruction is often inferior to primary reconstruction because the majority of patients have other knee problems such as arthritis, loss of a meniscus, deficiency of other ligaments, or bowed legs. In our experience, approximately 90% of patients have these problems. The goal of the operation is to alleviate pain and swelling with daily activities and return to low-impact activities in order to maintain an active lifestyle.
Patients who do not have arthritis, meniscus damage, bowed legs, or other ligament problems may have results similar to those reported after primary ACL reconstruction. Therefore, we recommend that ACL revision reconstruction be done early in athletically-active individuals or patients involved in strenuous occupations after failure of a prior procedure is detected. We do not recommend a trial of strenuous activity after a failed ACL reconstruction in these cases. This is because reinjuries and knee joint deterioration may occur in a manner similar to that observed in chronic ACL-deficient knees.
Dr. Frank Noyes and researchers at the NKI have published studies on the outcome of ACL revision reconstruction. In these studies, 140 patients who received either a patellar tendon allograft, patellar tendon autograft, or quadriceps tendon autograft were followed 2-7 years after the revision procedure. The studies were published in the Journal of Bone and Joint Surgery and in the American Journal of Sports Medicine.
- Similar results were found between patellar tendon autografts and quadriceps tendon autografts for knee stability (80% normal or nearly normal knee stability)
- Poorer results were found for allografts (67% normal or nearly normal knee stability)
- ACL revision surgery should be performed early after graft failure to avoid further joint damage.
- All attempts should be made to repair meniscus tears, because loss of meniscus function compounds knee problems.
- Bowed legs must be treated first with a high tibial osteotomy to correct the malalignment, because failure to do so carries a high likelihood of failure of ACL reconstructions.
- Associated knee ligament deficiencies must be surgically corrected with the ACL revision.
Why do PCL reconstructions fail?
While many clinical studies have been published on causes of failure of ACL reconstructions, few have investigated this problem after PCL reconstruction. We conducted the first study at the NKI to determine the most common factors which appeared to produce failure in a series of patients referred to us for revision PCL reconstruction. The factors include:
- Use of primary suture repair instead of a high strength graft substitute
- Failure to correct associated knee ligament ruptures or deficiencies, usually involving the posterolateral structures
- Failure to correct a bowed leg condition (varus osseous lower limb malalignment)
- Improper placement or orientation of the graft tunnels
- Traumatic reinjury
- A combination of any of the above factors
Shown below is an x-ray taken 1 year after a failed PCL and LCL/posterolateral reconstruction. The patient had a bowed leg and severe deficiency of the posterolateral structures. The bowed leg condition was not corrected and this caused both ligament reconstructions to fail.

Who are candidates for a PCL revision operation?
- Patients who have sustained complete failure of a prior PCL procedure as determined by > 10 mm of increased posterior tibial translation on manual testing or > 8 mm of increased posterior tibial translation on posterior stress x-rays
- Patients who have sustained complete failure of a prior PCL procedure and have symptoms or functional limitations with daily or sports activities

Who are NOT candidates for a PCL revision procedure?
- Patients that have partial function remaining of a prior PCL reconstruction
- Patients that have advanced knee arthritis (significant loss of joint space on x-rays)
- Patients who had a prior joint infection
- Patients who are obese (body mass index > 30)
- Patients who have bowed legs and will not undergo a high tibial osteotomy before or with the PCL revision reconstruction
- Patients who have severe muscle atrophy
- Patients with poor motivation or unrealistic expectations
- Patients with knee arthrofibrosis
- Patients who have deficiency of the posterolateral structures and will not undergo an associated posterolateral reconstruction with the PCL revision
What are the graft choices for PCL revision reconstruction?
The selection of the appropriate graft for PCL revision reconstruction remains controversial and there are incomplete clinical data to support definitive conclusions. Due to the inconsistent results reported from single-strand grafts, we prefer 2-strand graft constructs. Biomechanical and early clinical studies demonstrate that 2-strand grafts more closely replicate normal PCL behavior during knee motion and functional activities.
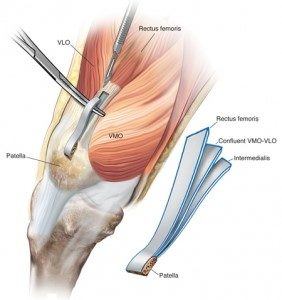
There are many different graft options for a 2-strand PCL revision reconstruction. One that we have used at the Noyes Knee Institute is the quadriceps tendon autograft which may be harvested from either from the injured knee or the contralateral knee (if previously harvested). This tendon is quite large and can be split to produce a 2-strand graft that is large enough to be placed through separate tunnels as shown below.
Another valid 2-strand graft option is the use of an Achilles tendon allograft.
What is the rehabilitation program after PCL revision reconstruction?
For patients who undergo PCL revision without an associated posterolateral reconstruction, the postoperative rehabilitation protocol may be found by clicking here.
For patients who undergo PCL revision with an associated posterolateral reconstruction, the postoperative rehabilitation protocol may be found by clicking here.
What are the results of PCL revision reconstruction?
The results expected from PCL revision are based on other operative procedures that are required, and the condition of the menisci and articular cartilage. The outcome of PCL revision reconstruction is usually inferior to primary reconstruction because the majority of patients have other knee problems such as arthritis, loss of a meniscus, deficient other ligaments, or bowed legs. In our experience, 80% of PCL revision cases have these problems. The goal of the operation in these patients is to alleviate pain and swelling with daily activities and return to low-impact activities in order to maintain an active lifestyle.
Patients who do not have arthritis, meniscus damage, bowed legs, or other ligament problems may have results similar to those reported after primary PCL reconstruction. However, further studies are required to determine the outcome of PCL revision based on the presence or absence of other knee-related problems.
Dr. Frank Noyes and researchers at the NKI published the first study on the outcome of PCL revision reconstruction in patients followed 2-7 years postoperatively. Improvement was noted in 80% for pain and in 87% for the patient perception of the overall knee condition. However, only 53% returned to light sports without problems. Adequate posterior knee stability was restored in 87%. The results were believed to be reasonable in the complex group of patients in whom other knee ligament reconstructions were required in 40% of the knees and a high tibial osteotomy was done in 20%.